System strategy isn’t about uniformity; it’s about intentional differentiation.
By Randall Zarin, MBA, MPH, CPA, Managing Director of Scout Strategy
In today’s healthcare landscape, hospital systems can no longer afford to operate as a loose federation of independent facilities. To thrive in a competitive, value-driven environment, health systems are evolving from holding companies – essentially groups of semi-autonomous hospitals sometimes grown through acquisition – into true operating companies that function as unified, strategic enterprises.
This transformation isn’t simply about governance; it touches every part of the organization: service lines, strategy, leadership, community presence, and physical infrastructure. Let’s explore what it takes to make the shift.
Building True System Service Lines
At the heart of the transition is the creation of system-wide service lines. Rather than each hospital maintaining its own specialty department (cardiology, oncology, etc.) in a silo, health systems are designing integrated, cross-campus service lines that:
- Share clinical protocols and pathways
- Leverage telemedicine and virtual consultation to extend specialty care
- Pool resources to invest in cutting-edge technology
- Align financial incentives across facilities
This structure allows for greater clinical quality, economies of scale, and consistency of patient experience across the system.
Defining a System-Wide Strategy
Operating companies must move beyond facility-specific strategic plans. A system strategy defines:
- What services should be offered where
- Which populations and markets to prioritize
- How growth, innovation, and financial goals will be achieved
- How the key Missions of clinical care, research and teaching will, or will not, be incorporated into the operating model
System strategy isn’t about uniformity; it’s about intentional differentiation. Some hospitals might be designated specialty hubs, while others focus on community-based acute care or ambulatory services. All decisions roll up to one system strategic vision not dozens of individual ones.
Consolidation and Clinical Re-Aggregation: Moving Beyond Redundancy
Transitioning to an operating company often requires consolidating duplicative services. Tough choices must be made about:
- Which locations will house cutting-edge surgical programs
- Where to centralize imaging or specialty outpatient care
- What legacy services no longer align with future system goals
Consolidation is always politically sensitive, especially when local communities or medical staff feel threatened. Transparent communication and a relentless focus on quality, access, and sustainability are critical to success.
Intentional clinical re-aggregation can be achieved, both internally in any one facility, and externally among geographically disparate locations, allowing for clinical economies of scale. Operational efficiency, increased quality and safety, and an enhanced experience for all stakeholders across the care continuum are the overwhelming advantages of consolidation and clinical re-aggregation. Of course, a deep understanding of the local demographic changes of the regional geography is foundational to guide the plan.
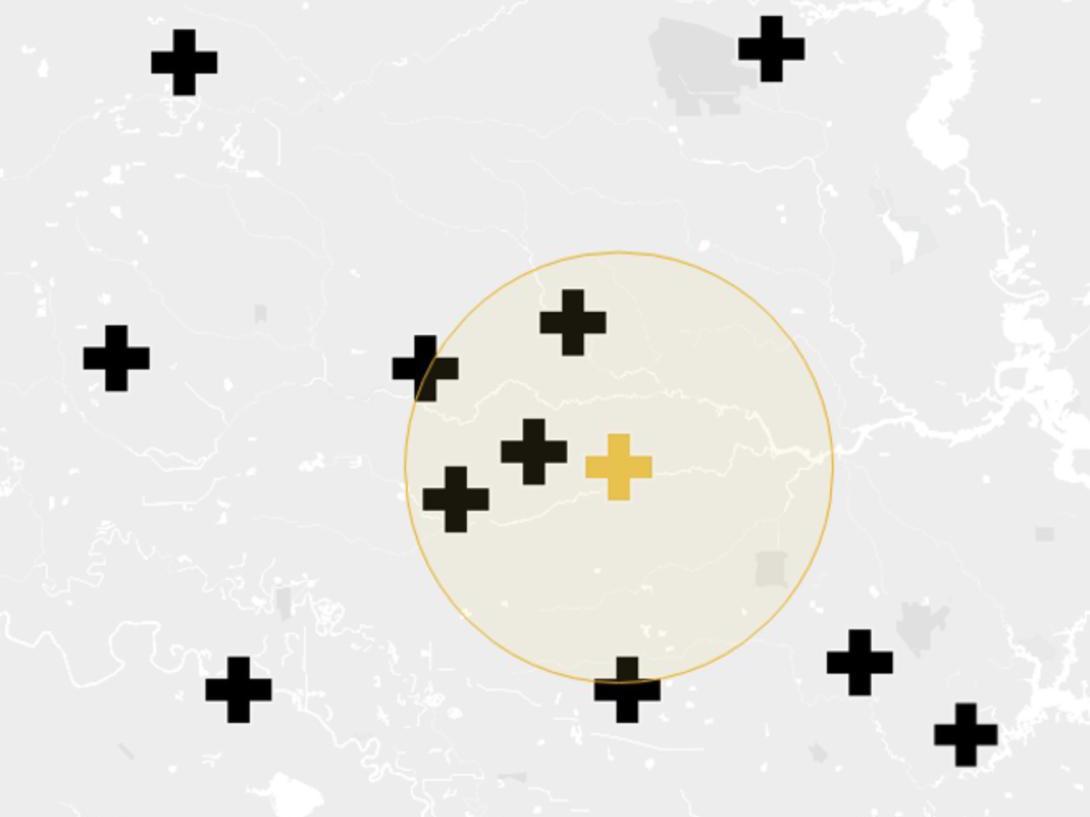
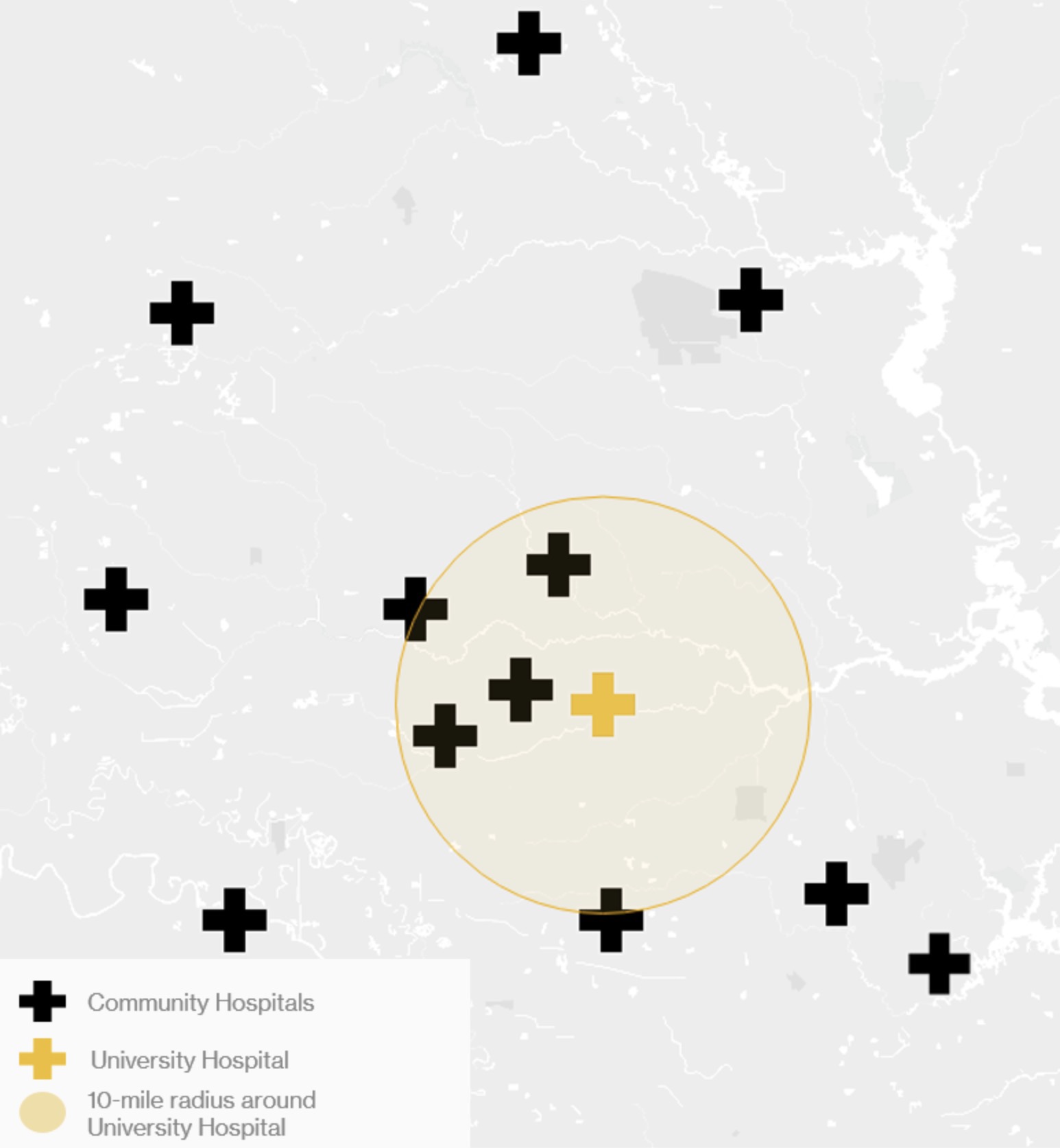
Community and University Hubs: Centerpieces of the System
Modern systems must recognize the importance of anchoring hubs:
- Community hubs serve as regional access points, often with a full continuum of care including urgent care, ambulatory surgery, and primary care networks.
- University hubs (for systems affiliated with academic institutions) represent centers for innovation, research, teaching centers for learners, and specialized, high acuity clinical care.
Both hubs should be intentionally developed and integrated into the system’s referral, educational, and research strategies; not allowed to grow independently based on local preferences.
Leadership Evolution: System and Local CEOs
The move to an operating company demands a new leadership model. Individual hospital CEOs evolve into market presidents or regional executives focused on executing system strategy locally. Their success is measured not solely by their own hospital’s performance, but by how well they contribute to system-wide goals.
Meanwhile, system executives (particularly the CEO, COO, Chief Medical Officer and Chief Strategy Officer) must lead with a unified vision and drive operational alignment across every facility, service line, and market.
Leadership structure must balance local agility with system accountability.
System Master Planning: Blueprint for the Future
Physical infrastructure must also evolve. System master planning rethinks:
- How to right-size and re-purpose existing campuses
- Where to invest in new outpatient and inpatient facilities
- How to optimize digital health and home-based care infrastructure
Master plans must be nimble, allowing for rapidly-evolving demographics, technology, and clinical innovation. Crucially, they must be rooted in system strategy, not historical precedent.
Conclusion
Transforming a hospital system from a holding company to an operating company isn’t just a structural change: it’s a cultural one. It demands clarity of purpose, strength of leadership, and the willingness to make bold, sometimes difficult decisions. But for systems that embrace the shift, the rewards are substantial: improved patient care, sustainable growth, stronger community presence, and a competitive edge in an increasingly complex healthcare environment.
The future belongs to systems that can act not as collections of hospitals, but as one organization with one mission.