
By Randall Zarin, MBA, MPH, CPA
Launching a new medical school is a monumental endeavor … one that requires proactive and meticulous planning, phased development, and a strategic vision for how education, research, and clinical functions will come together on an integrated campus. There are numerous planning categories to consider - the Built Environment being just one. The built environment plays a crucial role in the awareness and evolution of the school in the eyes of its stakeholders and prospective students, shaping not only the physical space, but also the institutional culture, academic success and community pride.
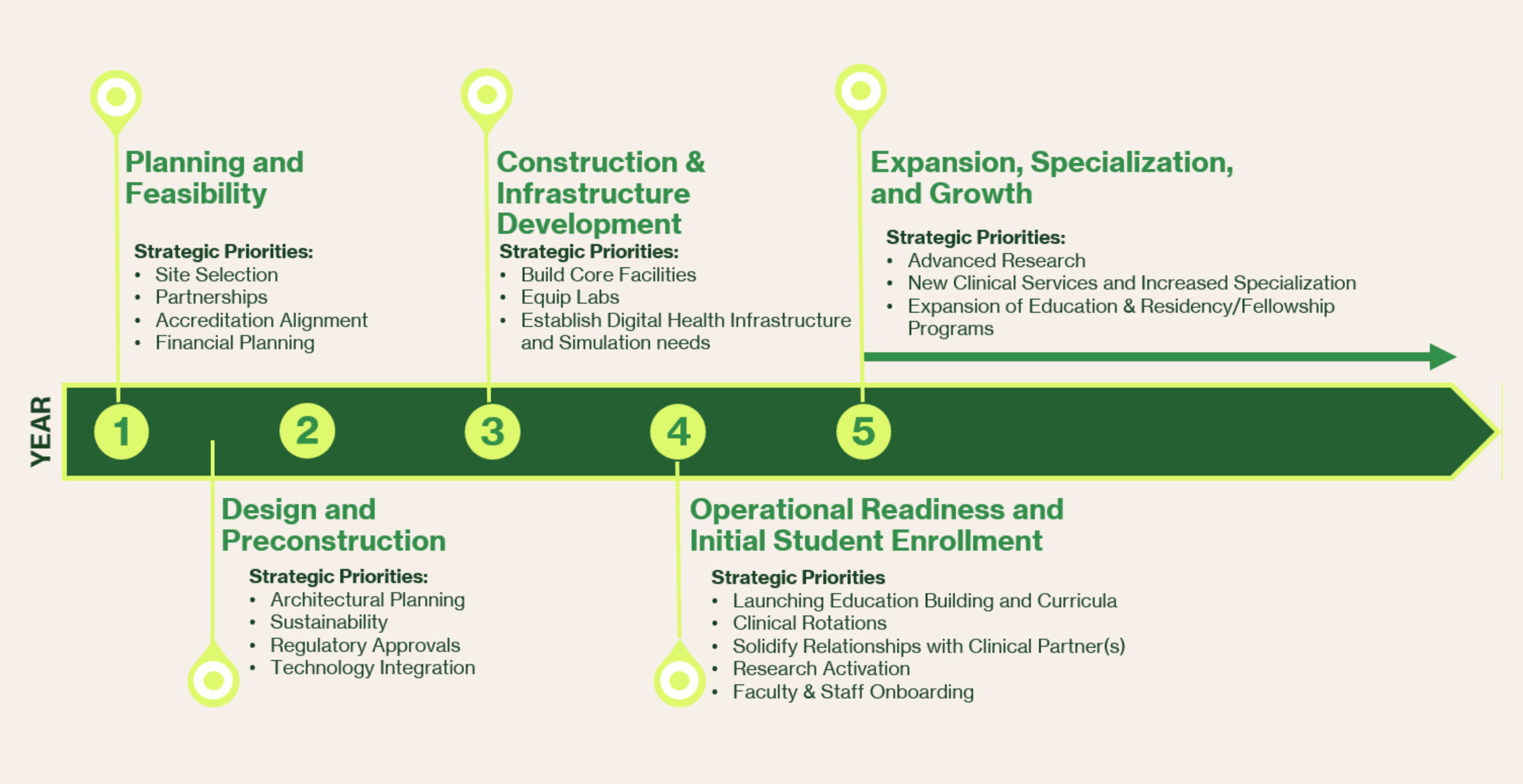
From its initial conception through full accreditation, the development of facilities follows a trajectory that aligns with accreditation milestones, educational needs, research aspirations, and clinical partnerships. Below, we explore the phased progression of a medical school’s physical infrastructure and how it evolves into a fully realized academic health campus from Day-1 to Years 10+.
Phase 1: Laying the Foundation (Pre-Accreditation – Day 1 to Year 1-2)
Primary Objective: Temporary and Adaptive Spaces
In the earliest days, before full accreditation and substantial funding are secured, the focus is on agility. Many new medical schools begin in leased or repurposed spaces, often within existing university buildings or clinical partner sites. These spaces accommodate foundational coursework and administrative operations while long-term plans for a dedicated medical school facility are developed.
Key Built Environment Priorities
- Classrooms and Simulation Labs: Early learning spaces prioritize flexibility, incorporating modular classrooms, clinical skills labs, and virtual anatomy solutions.
- Administrative Offices and Student Services: A compact footprint houses faculty, student affairs, and admissions teams, often co-located in multipurpose spaces.
- Research and Clinical Affiliations: Since standalone research and hospital facilities may not yet exist, early partnerships with local hospitals and research institutes provide initial access to clinical and scientific resources.
Accreditation Milestone:
During this phase, a school must demonstrate to accreditors that it has the necessary infrastructure and budget (sources of funding), whether leased or permanent, to support its first cohort of students. This includes facilities for basic sciences, clinical training, and student well-being.
Phase 2: Growth and Expansion (Years 2-5)
Primary Objective: Building a Permanent Campus
With initial cohorts progressing through the curriculum and accreditation steps advancing, attention turns to permanent facilities. This phase includes breaking ground on a dedicated medical education building and securing space for research and clinical expansion for the emerging faculty practice plan
Key Built Environment Priorities
- Medical Education Building: A purpose-built facility with lecture halls, simulation centers, standardized patient rooms, and interprofessional learning spaces.
- Anatomy and Research Labs: Wet labs for biomedical research and gross anatomy (or virtual) begin to take shape.
- Student Life and Wellness: As the student body grows, dedicated areas for student services, fitness, and mental health support become essential.
Clinical Integration
The school solidifies clinical training partnerships (UME), ensuring students have access to a variety of healthcare settings, from outpatient clinic sites to inpatient hospital facilities. Most schools develop early-stage clinical practice sites or faculty group practices to enhance hands-on learning opportunities.
Accreditation Milestone: Full Accreditation Site Visit Preparation
By this stage, accreditors assess the school’s ability to support students through graduation, including facilities for clinical training, student well-being, and research opportunities.
Phase 3: A Fully Functional Academic Medical Center - AMC (Years 5-10+)
Primary Objective: Expanding Clinical and Research Infrastructure
With full accreditation achieved and the first graduating class in practice, the school transitions from a developing entity to a fully operational academic medical center, including medical school facilities, acute and ambulatory clinical infrastructure and a functioning faculty practice plan.
Key Built Environment Priorities
- Academic Health Science Campus: This includes expanded research facilities, dedicated faculty practice clinics, and interprofessional education spaces for collaboration with nursing, pharmacy, and allied health programs and the AMC grows and evolves into an Academic Health Center (AHC).
- Affiliated or Owned Teaching Hospital: Some institutions develop or formalize ownership of a hospital to solidify their role as an integrated academic medical center.
- Technology-Enhanced Learning & Innovation Hubs: Dedicated spaces for AI-driven diagnostics and digital health innovations become a core part of the campus, including access to data centers (store and compute).
- Philanthropy-Driven Expansion: Endowed research centers and named buildings emerge as donor support grows.
Long-Term Vision – 11+ Years
At this stage, the medical school isn’t just a standalone entity, it’s a key driver of the healthcare workforce of the region, including research, and a driver of unique economic growth for the region. The built environment reflects this, with spaces that foster groundbreaking research, patient care, and innovative medical education.
Final Thoughts: More Than Just Buildings
The evolution of a medical school’s built environment is much more than a series of construction projects … it’s a reflection of the institution’s mission, values, and long-term impact on education, healthcare, and research. Each phase, from adaptive learning spaces to a full-fledged academic health center, contributes to a vision of excellence in medical education.
By thoughtfully designing the physical infrastructure in alignment with strategic growth, medical schools ensure that their campus not only meets accreditation standards but also becomes a thriving hub for the next generation of physicians, scientists, and healthcare leaders.